

RESEARCH ARTICLE
The impact of quality of glycemic control on exocrine pancreatic insufficiency syndrome in patients with type I diabetes mellitus: case-control study
Natalia Porcereanu1†*, Eugen Tcaciuc2†
1Endocrinology unit, Clinical Municipal Hospital “Sfanta Treime”, Chisinau, Republic of Moldova;
2Discipline of gastroenterology, Department of internal medicine, Nicolae Testemițanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova.
Corresponding author:
Natalia Porcereanu, endocrinologist
Endocrinology unit
Clinical Municipal Hospital “Sfanta Treime”
11, Alecu Russo str., Chisinau, Republic of Moldova, MD-2068
e-mail: nataliaporcereanu@yahoo.com
Short title: Type 1 diabetes mellitus and pancreatic exocrine insufficiency
What is not known yet, about the topic
The cause of the increased prevalence of pancreatic exocrine insufficiency (PEI) in patients with diabetes mellitus (DM) and predisposing factors is insufficiently elucidated.
Research hypothesis
There may be a correlation between microvascular complications of DM and PEI, the latter being a consequence of autonomic diabetic neuropathy, which could be favorably influenced by satisfactory glycemic compensation.
Article`s added novelty on this scientific field
It has been shown that the existence of microvascular complications of DM and the compensation of unsatisfactory DM have an important predictive value for the development of PEI in patients with type 1 DM.
ABSTRACT
Introduction. Type 1 diabetes is an autoimmune metabolic pathology that affects young people, with significant consequences on quality of life, morbidity and mortality. In addition to well-known microvascular complications, the therapeutic management of which is guided by a solid scientific data base, there are pathological conditions related to DM less investigated. PEI has a high prevalence in DM patients even in the absence of an organic pathology of the pancreas. Deregulation of micronutrient digestion and absorption processes as a consequence of undetected and untreated PEI results in altering the quality of life of patients and adversely affects the prognosis of people with DM. The purpose of the research was to elucidate the interrelationships between PEI and diabetic microvascular complications as well as the degree of compensation of glucose metabolism in patients with DM and PEI.
Materials and methods. A case-control study was performed on 138 patients with Type 1 DM without organic digestive pathology. The baseline (PEI) group consisted of 67 patients with type 1 DM and PEI (faecal pancreatic elastase ≤200 μg/g), and the non-PEI group consisted of 71 patients with type 1 DM with intact pancreatic exocrine function. The microvascular complications of DM have been evaluated such as: autonomic cardiovascular diabetic neuropathy, diabetic nephropathy, diabetic retinopathy, peripheral diabetic neuropathy. The survey used included the anamnestic data: age at the time of research, age at onset DM, DM term; regular glycemic control, systemic adjustment of insulin doses, frequency of acute diabetic complications (hypoglycaemic and ketoacidosis conditions). biochemical parameters: peptide C, glycated hemoglobin (HbA1c) and basal glycaemia were evaluated.
Results. A higher prevalence of microvascular complications of DM in the PEI group was demonstrated compared to the non-PEI group (p<0.01). Significant statistical differences were obtained between the research groups in terms of age of the patients at the time of research, DM, these values being higher in the PEI group (p<0.05). The age of patients at the onset of DM did not correlate with exocrine dysfunction of the pancreas. Patients in the PEI group had a poorer glycemic compensation compared to the non-PEI group, glycated hemoglobin (8.36±0.17 vs. 7.80±0.13 mmol/l, p<0.05) and basal glycaemia being higher in the PEI group (8.41±0.33 vs. 7.21±0.19 mmol/l; p<0.01).
Conclusions. Exocrine pancreatic insufficiency in patients with DM is one of the main causes of autonomic diabetic neuropathy. This contributes to the unsatisfactory compensation of DM and poor glycemic control. There is a dependence between PEI and microvascular complications of DM and the duration of diabetes.
Keywords: diabetes mellitus, peptide C, glycated hemoglobin, exocrine pancreatic insufficiency, autonomic diabetic neuropathy.
INTRODUCTION
Over the past decades, several aspects of the interactions of the exocrine and endocrine portion of the pancreas have been elucidated, a phenomenon known as the "insulin-acinar axis". Recent research on pancreatic tissues has demonstrated the influence of insulin hormones on exocrine pancreas, the first such research being performed in patients with DM. PEI is a pathological condition commonly found in patients with DM in the absence of organic pancreas damage. The incidence of PEI was detected in 50% of patients with type 2 DM and in 40-73% of patients with type 1 DM [1].
Some research demonstrates the association of PEI with the long duration of DM. Several studies confirm PEI's dependence on early DM and gender onset, with a higher prevalence of PEI in males, although other research has contradictory results. Data on the effectiveness of glycemic control are also quite controversial.
The local trophic effect of insulin has long been considered one of the main mechanisms of PEI in patients with type 1 DM. A reduction in pancreas dimensions in patients with DM has been described, this reduction correlates with FEC-1 reduction, suggesting a link between diminishing pancreas size and exocrine function [2]. Computed morphometry of the exocrine pancreas demonstrates atrial atrophy, reducing the size of the acinar cells. The possible lack of the trophic effect of insulin is an important mechanism of involution of the exocrine pancreatic portion. Decreasing endogenous neurohormonal stimulation and alteration of enteropancreatic reflexes as a result of autonomic diabetic neuropathy could be the main cause of PEI in patients with DM. Diabetic neuropathy is a common complication of DM affecting up more than 50% of patients and is more commonly associated with type 1 DM than type 2 DM (60% for type 1 and 35% for type 2). In patients with autonomic neuropathy by affecting enteropancreatic reflexes, the pancreatic secretion reaction to cholecystokinin and its analogues is deregulated. In patients with DM, there is a difference in the excretion of pancreatic polypeptide, intestinal hormones (motilin), vasoactive intestinal peptides, which influence pancreatic exocrine function. Deregulation in the activity of the enteric nervous system and Cajal interstitial cells, independent of the autonomic nervous system, and myopathy of smooth muscle cells are another consequence of DM. Several researches demonstrate a reduction in the number of Cajal interstitial cells in the stomach, small intestine and colon in patients with DM [3]. Diabetic gastroparesis is the most common manifestation of autonomic digestive neuropathy. The delay in gastric emptying occurs in 25-50% of patients with type 1 DM with a disease term greater than 10 years. Radioisotope tests reveal delay in gastric emptying in 30-50% of patients with type 1 or 2 DM with a long term of evolution. It coexists with other manifestations of autonomic neuropathy: orthostatic hypotension, tachycardia. The degree of impairment is not commensurate with symptomatology, because there are asymptomatic patients with pronounced gastroparesis [4].
The crucial importance of pancreatic exocrine function is related to maldigestion and malabsorption that may occur as a result of an untreated PEI [5]. PEI has as a consequence nutrient deficiency syndrome, a multitude of trophic changes as a result of protein and vitamin deficiency, lipid, carbohydrates, minerals metabolism disorders with important pathophysiological consequences [9]. These include morpho-functional changes in digestive organs (atrophy mucous membranes, alteration of the microbial flora content), lability of blood circulation, immunodeficiency, and endocrine disruptions [6]. Together with known cardiovascular risk factors such as tobacco and high blood pressure, PEI is considered an independent risk factor associated with increased cardiovascular events in patients with chronic pancreatitis and PEI [7]. The outcomes of the EuroOOPS prospective cohort study demonstrated the importance of nutrition status and nutritional management of hospitalized patients. NRS-2002 (Nutritional Risk Screening) was used to screen for malnutrition and assess the risk of progression of malnutrition in hospitalized patients as well as to identify associations between denaturing and clinical outcomes. Patients with increased NRS-2002 nutritional risk had a longer duration of hospitalization (9 days versus 6 days), developed more complications during hospitalization (30.6% vs. 11.3%) and had a higher rate of hospitalization mortality (12.1 vs. 1%) [8]. The importance of nutritional status and nutritional markers is confirmed as predictors of survival in haemodialysis patients [10].
Retrospective studies investigated the influence of Type 1 DM on mortality, the effect of DM on the years of life lost (YLL) was compared with the effect of other pathologies on YLL. The Australian study, which included patients with type 1 DM with a starting age less than 45 years, between 1997 and 2010, showed a reduction in life expectancy compared to the general population by 12.2 years (11.6 years for men and 12.5 years for women) [11]. The 1984-2000 data from the National Health Interview Surveys (US) show that the life expectancy of patients with type 1 DM diagnosed at 10 years is reduced by 19 years [12].
Elucidation of the etiopathogenetic aspects of PEI and the risk factors associated with this disorder in patients with type 1 DM would allow for the optimization of the therapeutic course of patients with type 1 and associated PEI patients, contributing to improving the quality of life and increasing life expectancy in patients with type 1 DM [13].
MATERIAL AND METHODS
We performed a case-control study that included patients with Type 1 DM hospitalized in the Endocrinology unit of the Clinical Municipal Hospital "Sfanta Treime" during the 2014-2016 period.
The research protocol was approved by the Research Ethics Committee of the Nicolae Testemitanu SUMPh (minutes no. 20 from 10 of March, 2014, Chairman of the REC – Prof. Mihail Gavriliuc, PhD). Participation in the study was voluntary, based on the informed signed consent.
The inclusion criteria were: Type 1 DM (diagnosed according to ADA 2013 criteria), DM term longer than 3 years. Exclusion criteria were: serious somatic state, unbalanced DM (hyperglycaemia or hypoglycaemia), primary digestive system pathology, alcohol abuse, smoking, pregnancy.
The research included 138 subjects with type 1 DM: 85 (61.6%) men and 53 (38.4%) women. The PEI group consisted of 67 patients with type 1 DM and PEI, and the non-PEI group consisted of 71 patients with type 1 DM with intact pancreatic exocrine function. Patients in the research group had a faecal elastase (FEC-1) value of ≤200 μg/g and patients in the pancreatic exocrine pancreatic group had FEC-1 >200 μg/g. According to recent years, FEC-1 assessment is a test with high specificity and sensitivity, performed by the immunoenzymatic method. Specificity of the method is considered 90-100% and sensitivity 93-98% [14].
Enrolled patients were questioned. The primary data recording sheet included information on the regular glycaemic control and adjustment of insulin doses, frequency of acute complications of DM – hypoglycaemia and hyperglycaemia. Basal blood glucose and glycated haemoglobin (HbA1c) were evaluated.
The presence of microvascular complications of DM has been investigated: peripheral diabetic neuropathy (PDN), diabetic retinopathy (DR), diabetic nephropathy, autonomic cardiovascular neuropathy (ACN). The Toronto Score (TCNS) was used to diagnose PDN and assess its severity. Clinical score evaluation allows correlation with structural lesions of the peripheral nerves [15]. Each score component was rated 0-1 points depending on presence or absence, except for reflexes that were rated 0, 1 or 2 points (normal, low or absent). The score of 0-5 points signifies the absence of PDN, 6-8 points denotes light PDN, 9-11 points in the case of moderate PDN, and over 12 points attests to severe PDN. The maximum score may be 19 points. For the ACN evaluation, was used the vegetative functional tests known as Ewing's test battery: variation of heart rate at hyperpnoea, heart rate response to orthostatism, variation of heart rate at Valsalva manoeuvre, blood pressure response to orthostatism, and blood pressure response to isometric hand contraction.
For the diagnosis of diabetic retinopathy the ophthalmoscopic examination was performed by the ophthalmologist and the research was performed in the Ophthalmology unit of the CMH "Sfanta Treime". The ophthalmoscopic examination allowed DR staging according to the International Council of Ophthalmology (ICO) criteria: minimal, moderate or severe non-proliferative diabetic retinopathy; proliferative diabetic retinopathy [16].
Microalbuminuria was evaluated in the subjects included in the research by qualitative testing, the positive value of microalbuminuria was considered a criteria for estimating the amount of nictemeral protein in the urine. Renal function was evaluated using the estimated glomerular filtration rate [17]. Staging of chronic kidney disease was performed according to the KDOQI (Kidney Disease Outcomes Quality Initiative) classification that sets five stages for chronic kidney disease in the Practical Guide to Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification and Stratification”. The glomerular filtration rate (GFR) was determined by the formula MDRD.
Upper gastrointestinal tract radiography was performed to evaluate gastric and intestinal motility. The organs of the abdominal cavity were examined by ultrasound. This allowed the assessment of the pancreas dimensions as well as the examination of the digestive organs in order to detect a possible organic pathology and to highlight possible morphological criteria specific to the chronic pancreatitis [18]. The abdominal ultrasonography of the abdomen à jeun, after a minimum 8-hour food rest period, allowed the identification of slowing the stomach passage by detecting stomach contents.
We investigated the value of peptide C in the blood in patients included in the research. The peptide C represents the middle portion of the insulin and results from the proteolytic cleavage of the proinsulin precursor molecule. Peptide C evaluation is a relevant method of assessing endogenous insulin secretion in patients with type 1 DM [19].
Category data are presented as an absolute and relative value. The statistical test applied for comparison between groups: χ2. Continuous type data are presented as average and standard error. Applied statistical test: two tailed unpaired t-Student test. The degree of correlation between two variables was estimated by Pearson criterion. A p<0.05 was considered statistically significant. The statistical analysis was performed with the SPSS v. 22 software.
RESULTS
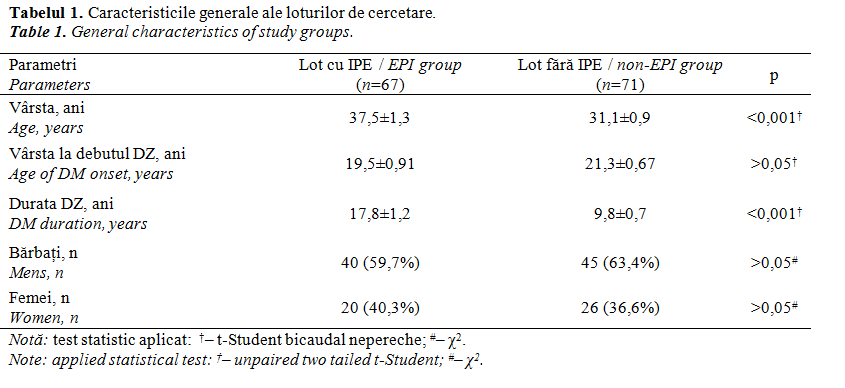
Patients in the IPE group had an average DM duration of 17.8±1.3 years, while subjects in the non-PEI group had an average disease duration of 9.8±0.7 years. Patients without PEI were younger (31.1±0.90 years) than those with PEI (37.5±1.3 years), the average age being 34.2±0.8 years. The average age at onset of DM was 20.5 years (±0.8), in the IPE group, patients were younger (19.6±1.1 years) compared to the non-PEI group (21.3±1.0 years), with no significant statistical difference. No statistically significant gender differences were found between the groups studied. Table 1 presents the general characteristics of the research batches.
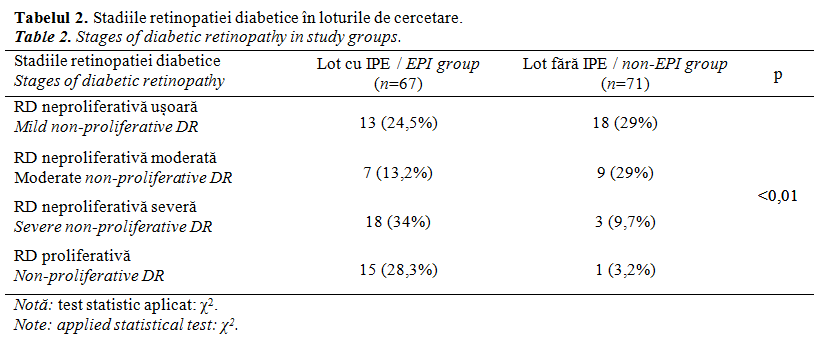
 Ophthalmoscopic examination allowed the diagnosis of diabetic retinopathy in the research groups. A number of 53 (79.1%) persons in the base group had DR-specific retinal changes. In the non-PEI group, retinal ophthalmoscopic changes were detected in 31 (43.7%) patients. One patient in the non-PEI group had proliferative DR, and in the research group there were 15 patients with proliferative DR. The majority of subjects with light non-proliferative DR (18 patients) and moderate non-proliferative DR (9 patients) belonged to the non-PEI group, while patients with predominantly advanced DR status belonged to the research group (18 patients with severe non-proliferative DR and 15 patients with Proliferative DR). DR’s stages were shown in the research batches in Table 2.
Ophthalmoscopic examination allowed the diagnosis of diabetic retinopathy in the research groups. A number of 53 (79.1%) persons in the base group had DR-specific retinal changes. In the non-PEI group, retinal ophthalmoscopic changes were detected in 31 (43.7%) patients. One patient in the non-PEI group had proliferative DR, and in the research group there were 15 patients with proliferative DR. The majority of subjects with light non-proliferative DR (18 patients) and moderate non-proliferative DR (9 patients) belonged to the non-PEI group, while patients with predominantly advanced DR status belonged to the research group (18 patients with severe non-proliferative DR and 15 patients with Proliferative DR). DR’s stages were shown in the research batches in Table 2.
Retinal oedema was detected in 26 of the patients enrolled in research, representing 18.8% of the total, with a significant prevalence in the PEI group compared to the non-PEI group (32.8% vs. 5.6%, p<0.001).
The presence of microalbuminuria and proteinuria was found in 79 (57.2%) patients with a significant predominance in the PEI group, where the prevalence of microalbuminuria and proteinuria was 71.6% (48 patients). In the non-PEI group, proteinuria was detected in fewer patients (31 patients or 43.7%, p <0.01). In the PEI group, patients had higher protein values in the urine compared to the average proteinuria level in the non-PEI group (0.07±0.017 g/24 hours vs. 0.50±0.12 g/24 h, p<0.01). A poor negative correlation between proteinuria and FEC-1 (r=-0.263; p<0.01) was found.
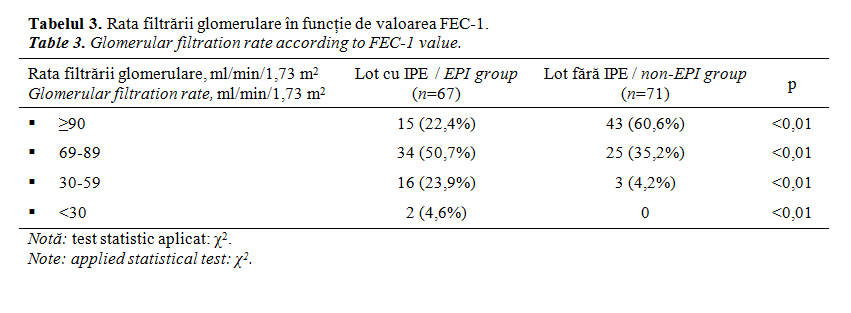
Staging the DN according to the glomerular filtration rate (GFR) in the classification KDOQI allowed a strong correlation of DN and PEI with a significant predominance of advanced DN stages in PEI patients (p<0.001). Eighty patients of the total number enrolled in research, had GFR below 90 ml/min/1.73 m2. In the non-PEI group predominant GFR values were above 80 ml/min/1.73 m2. The advanced stages of DN with GFR <60 ml/min/1.73 m2 were found in 21 patients: 18 (26.9%) patients in the PEI group (of whom 2 patients had end-stage chronic kidney disease (CKD) and were in chronic haemodialysis treatment and 3 (4.2%) patients from the non-PEI group, with CKD III stage KDOQI. The distribution of patients from the GFR-dependent research groups according to KDOQI staging of CKD is shown in Table 3.
ACN was detected in 94 (68.2%) persons from the number included in the research. Most ACN subjects were part of the PEI group (58.1% vs. 49.3%, p<0.001). Severe ACN recorded 17 (25.4%) patients in the research group and 3 (4.2%) patients in the non-PEI group. Moderate ACN was detected in 27 (40.3%) subjects in the research group and 9 (12.7%) subjects in the non-PEI group. Only 8 (11.9%) patients in the research group did not report ACN, while in the non-PEI group the proportion of patients without ACN was significantly higher (36 persons, 47.9%).
We obtained a Toronto score of 8.0±0.71 points assessing peripheral diabetic neuropathy in patients in the PEI group, which corresponds to a moderate-light peripheral neuropathy. The score for the non-PEI group was 2.2±0.37 points, scores between 0 and 5 points signifying the absence of peripheral neuropathy. The difference between the Toronto scores of the research groups was statistically significant (p<0.001).
Evaluation of autonomic digestive neuropathy was performed by gastric motility research and gastric hypokinesia signs. Superior digestive radioscopy with barite mass allowed the detection of gastric emptying of the barite mass at 40 (35.7%) subjects. In the PEI group there were 33 persons with prolonged gastric emptying time, and in the non-PEI group there were 7 persons (63.5% vs. 11.7%, p<0.001). The gastric content was found in 21 (18.6%) patients, the majority (15 patients) being part of the PEI group; in the non-PEI group only 6 patients had signs of gastric emptying (28.3% vs. 10%, p<0.05). Hypomotor gastric dyskinesia was detected at 40 (35.4%) patients of the investigated groups. In the PEI group there were 32 (60.4%) patients with hypomotoric dyskinesia and in the non-PEI group there were 8 (13.3%) patients with hypomotoric dyskinesia (p<0.01).
Ultrasound of the abdominal organs allowed the gastric contents to be displayed on an empty stomach after a minimum of 8 hours of resting. Signs of slowing gastric emptying were detected at 20 (15.2%) patients, with a higher prevalence of PEI patients – 14 (22.2%) patients of the PEI group, compared to the non-PEI group – 6 (8.7%) patients (p<0.05).
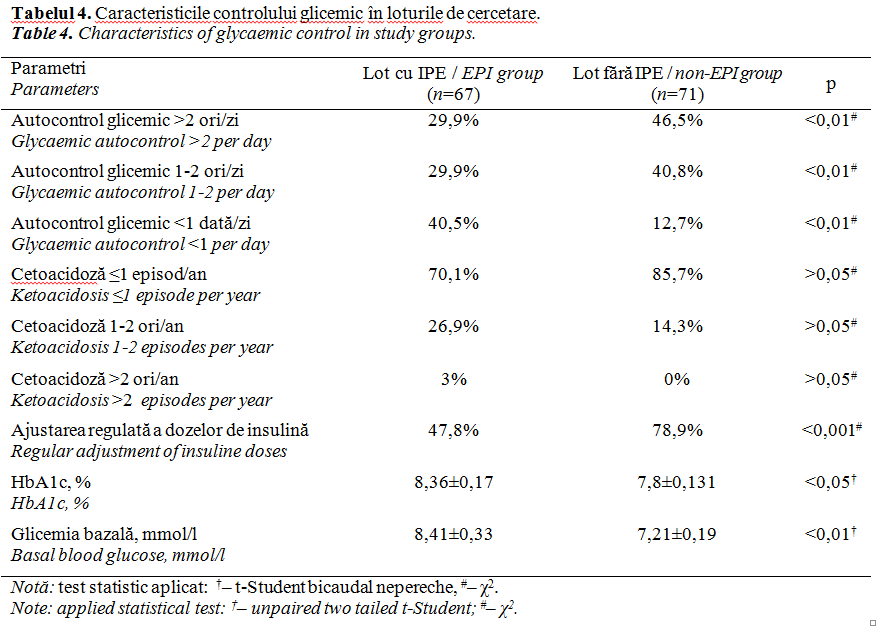
Table 4 illustrates glycaemic control characteristics in the research batches. The average level of glucose was 7.79 ± 0.194 mmol/l. In the research group we recorded higher baseline blood glucose levels compared to the non-PEI group (8.41±0.33 mmol/l vs. 7.21±0.19 mmol/l, p<0.01). The correlation between basal and baseline FEC-1 was poorly negative (r=-0.227; p<0.01).
A lower glycaemic control in the research group was also confirmed by HbA1c values, which were higher compared to the non-PEI group (p<0.05). The average level of HBA1c in the baseline consisted of 8.36±0.17%, and the HbA1c of 7.8±0.131% was determined in the non-PEI group. The mean HbA1c score at the patients included in the study was 8.09±0.1%. There was a poor negative correlation between HbA1c and FEC-1 (r=-0.255; p<0.01).
Eighty-eight (63.8%) subjects from the non-PEI group confirmed the adjustment of the insulin dose (p<0.001). The 78.9% of the patients (56 persons) of the non-PEI group are adjusting the insulin dose. Of the baseline, 32 (47.8%) people adjusted the insulin dose.
Fifty-three (38.4%) of the patients included in the research reported that they did glycaemic self-control more than 2 times a day. The higher proportion of patients with more intense glycaemic control was the non-PEI group compared to subjects in the PEI group (46.5% vs. 29.9%, p<0.01). There were 29.9% of patients in the research group and 40.8% of the non-PEI group who reported glycaemic control 1-2 times a day. The absence of daily glycaemic control, with a frequency of several times a week, was reported by 40.5% of the patients in the research group and 12.7% of the non-PEI group.
Rare episodes of ketoacidosis, less than 1 episode/year, or absence, reported 107 patients (78.1% of the total). The frequency of rare ketoacidosis episodes in the research group was 70.1%, while in the non-PEI group – 85.7%. More frequent episodes of ketoacidosis, 1-2 times a year, reported 18 (26.9%) patients in the IPE group and 10 (14.3%) patients in the non-PEI group. Frequent episodes, more than 2 episodes/year, reported only 2 (3%) patients, being part of the research group.
The mean C-peptide was 0.352±0.014 ng/ml and we obtained a higher value in the non-PEI group (0.391±0.02 ng/ml) compared to the PEI group (0.314±0.019 ng/ml, p<0.01).
DISCUSSION
PEI is a pathological condition commonly encountered at patients with DM, there is more controversial data on the prevalence and pathogenesis of this complication. Patients with DM have multiple conditions predisposed to PEI: exocrine pancreas atrophy as a result of reducing the trophic effect of high local insulin concentrations and microangiopathy; premature enzyme degradation as a result of reduced contact time in intestinal dysmotility and overgrowth syndrome; autoimmune disorder of the exocrine pancreas. One of the most important causes would be the reduction of endogenous neurohormonal stimulation and the alteration of entero-pancreatic reflexes as a result of autonomic diabetic neuropathy.
At patients in the PEI group, we found a higher prevalence of DM complications. The presence of PEI is correlated with peripheral diabetic neuropathy, a more advanced degree of peripheral neuropathy being associated with a more significant reduction in FEC-1. A more advanced stage of diabetic nephropathy and higher proteinuria was found in the batch of PEI patients. There was a predominance of severe ACN grades in the PEI group and the predominance of severe DR in the PEI group.
Examination of digestive transit by radioscopy demonstrated slowing of gastric emptying at patients in the PEI group compared to the non-PEI group. The abdominal ultrasound examination allowed a predominant gastric stasis to be found in the PEI group. These data allow us to establish a link between PEI and microvascular complications of type 1 DM, PEI being a consequence of autonomic diabetic neuropathy or a DM complication.
The main role in the etiopathogenesis of diabetic neuropathy is chronic hyperglycaemia. This statement was supported by a number of large-scale applications. Patients in the PEI group had glycaemic control parameters indicating a lower DM compensation compared to the non-PEI group. Incorrect glycaemic control and non-adjustment of insulin doses are the premises of insufficient glycaemic control. Good glycaemic control is associated with reducing the rate of diabetic microvascular complications. Patients in the PEI group had a reduced frequency of glycaemic self-control compared to the non-PEI group. Higher HbA1c at the base group confirms less satisfactory metabolic compensation. The HbA1c <7% is recommended for most patients with type 1 DM for the prevention of DM complications, and some patients who are at risk of hypoglycaemia may be recommended for HbA1c <6.5% [21]. These ADA recommendations from 2017 are based on the results of the DCCT prospectively controlled clinical trial, and the EDIC study has confirmed the persistence of the microvascular benefit of intensive glycaemic control in patients with type 1 DM [20].
CONCLUSIONS
PEI is a pathological condition with significant prevalence at patients with type 1 DM, often asymptomatic. The importance of early diagnosis of this deficiency results from the negative impact of the PEI on the nutritional and metabolic balance with long-term adverse effects.
Patients with long-term type 1 DM, with diabetic microvascular complications and poor glycaemic control are those who should be investigated for PEI detection, and the FEC-1 assessment is a simple and accessible diagnostic method. Substitution enzyme therapy indicated when needed in severe PEI cases would bring long-term benefits, improving quality of life and increasing life expectancy.
Declaration of conflicting interests
Nothing to declare.
Authors` contribution
Both authors contributed equally to the elaboration of the manuscript. The final version has been read and approved by both authors.
REFERENCES
- Mohapatra S., Majumder S., Smyrk T., Zhang L., Matveyenko A., Kudva Y., Chari S. Diabetes mellitus is associated with an exocrine pancreatopathy: conclusions from a review of literature. Pancreas, 2016; 45: 1104-110. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5833980.
- Philippe M., Benabadji S., Barbot-Trystram L., Vadrot D., Boitard C., Larger E. Pancreatic volume and endocrine and exocrine functions in patients with diabetes. Pancreas, 2011; 40 (3): 359-63. https://doi.org/10.1097/MPA.0b013e3182072032.
- Long Q., Fang D., Shi H., Luo Y. Gastro-electric dysrhythm and lack of gastric interstitial cells of cajal. World J. Gastroenterol., 2004; 10: 1227-1230.
- Kong M., Horowitz M., Jones K., Wishart J., Harding P. Natural history of diabetic gastroparesis. Diabetes Care, 1999; 22: 503-507.
- Keller J., Layer P. Human pancreatic exocrine response to nutrients in health and disease. Gut, 2005; 54: 61-28.
- Kim M., Basharat A., Santosh R. et al. Reuniting overnutrition and undernutrition, macronutrients, and micronutrients. Diabetes Metab. Res Rev., 2018; e3072. https://doi.org/10.1002/dmrr.3072.
- de la Iglesia D., Vallejo‐Senra N., López‐López A., Iglesias‐Garcia J., Lariño‐Noia J., Nieto‐García L., Domínguez‐Muñoz J. Pancreatic exocrine insufficiency and cardiovascular risk in patients with chronic pancreatitis: a prospective, longitudinal cohort study. Journal of Gastroenterology and Hepatology, 2018; https://doi.org/10.1111/jgh.14460.
- Sorensen J., Kondrup J., Prokopowicz J., Schiesser M., Krähenbühl L., Meier R. et al. EuroOOPS: an international, multicentre study to implement nutritional risk screening and evaluate clinical outcome. Clin. Nutr., 2008; 27: 340-349.
- Pongprasobchai S. Maldigestion from pancreatic exocrine insufficiency. J. Gastroenterol. Hepatol., 2013; 28 (4): 99-102.
- Leavey S., Strawderman R., Jones C., Port F., Held P. Simple nutritional indicators as independent predictors of mortality in hemodialysis patients. Am. J. Kidney Dis., 1998; 31: 997-1006.
- Huo L., Harding J., Peeters A., Shaw J., Magliano D. Life expectancy of type 1 diabetic patients during 1997-2010: a national Australian registry-based cohort study. Diabetologia, 2016; 59: 1177-1185.
- Narayan K., Boyle J., Thompson T., Sorensen S., Williamson D. Lifetime risk for diabetes mellitus in the United States. JAMA, 2003; 290: 1884-1890.
- Dominguez-Muñoz J. Diagnosis and treatment of pancreatic exocrine insufficiency. Curr. Opin. Gastroenterol., 2018; 34 (5): 349-354.
- Vanga Rohini R. et al. Diagnostic performance of measurement of fecal elastase-1 in detection of exocrine pancreatic insufficiency: systematic review and meta-analysis. Clinical Gastroenterology and Hepatology, 2018; 16 (8): 1220-1228.
- Bril V., Perkins B. Validation of the Toronto Clinical Scoring System for diabetic polyneuropathy. Diabetes Care, 2002; 25 (11): 2048-52.
- International Council of Ophthalmology (ICO) Guidelines for Diabetic Eye Care, 2017.
- Kidney Disease: Improving Global Outcomes Group (KDIGO) Work GroupKDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl, 2013; 3:1-150.
- Ito T., Ishiguro H., Ohara, H. et al. Evidence-based clinical practice guidelines for chronic pancreatitis 2015. J. Gastroenterol., 2016; 51: 85. https://doi.org/10.1007/s00535-015-1149-x.
- Palmer J., Fleming G., Greenbaum C., Herold K., Jansa L., Kolb H., Lachin J., Polonsky K., Pozzilli P., Skyler J., Steffes M. C-peptide is the appropriate outcome measure for Type 1 diabetes clinical trials to preserve β-cell function. Diabetes, 2004; 53 (1): 250-264.
- Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Study Research Group Intensive diabetes treatment and cardiovascular outcomes in type 1 diabetes: the DCCT/EDIC study 30-year follow-up. Diabetes Care, 2016; 39: 686-693.
- Chamberlain J., Kalyani R., Leal S., Rhinehart A., Shubrook J., Skolnik N., Herman W. Treatment of type 1 diabetes: synopsis of the 2017 American diabetes association standards of medical care in diabetes. Ann. Intern. Med., 2017; 167: 493-498. https://doi.org/10.7326/M17-1259.