

RESEARCH ARTICLE
Prevalence of malocclusions in children with special needs: prospective, descriptive study
Cristina Poștaru1*, Svetlana Melnic1, Mihail Postnikov2, Diana Uncuța1
1Chair of propedeutical stomatology “Pavel Godoroja”, Nicolae Testemitanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova;
2Chiar of pediatric dentistry, State University of Medicine, Samara, Russian Federation.
Corresponding author:
Cristina Postaru, PhD fellow
Chair of propedeutical stomatology „Pavel Godoroja”
University Dental Clinic
1A, Mihai Viteazu str., Chisinau, Republic of Moldova, MD-2004
e-mail: c_railean@yahoo.com
Short title: Prevalence of malocclusions in children with special needs
What is not known yet, about the topic
The prevalence of malocclusion is not known in children in three reference plans in association with auditory, visually and physically handicapped patients.
Research hypothesis
Children with auditory, visually and physically disorders show malocclusion in significantly different proportions.
Article’s added novelty on this scientific topic
The estimated prevalence of dentomaxillary abnormalities in children with special needs was 67.5%. Dentomaxillary anomalies in the sagittal plane were found in 20.4% of children, vertically – in 53.4% and transversely – in 26.2% of children. According to age, the most affected were the children of 12-15 years (33.7%), following those of 9-12 years (28.3%), then – those of 7-9 years (22.6%).
ABSTRACT
Introduction. Children with special needs, especially with auditory, visually and physically (cerebral palsy) impairment are considered children with a health problems, especially, in the process of social adaptation, due to mental or physical conditions. Determining the prevalence of malocclusion in these children that could then have a unique mechanism in the onset of malocclusions is less studied.
Material and methods. Were examined, with permission of Ministry of Health of the Republic of Moldova and of the Municipal direction for the protection of children’s rights 2057 of children with special needs (physically/motor, visually, auditory impairments) from different temporary placement centers, auxiliary schools and special gymnasiums from Hancesti, Soroca and Orhei districts. Duration of the research: 2012-2014 years. Age of the children was between 7 and 15 y.o. Clinical examination of children included: disposable dental mirror, chemical pencil, wooden spatula, caliper, portable light. Descriptive statistic.
Results. The prevalence of malocclusions in children with special needs was 1388/2057 cases (67.5%) In sagittal plan malocclusion was associated in 283 (20.4%) children, in vertical plan – 741 (53.4%) children, in a transversal plane – in 364 (26.2%). Mostly, malocclusion has been detected in physically handicapped children – 309/524 (26.2%) in vertical plan, in visually handicapped children – 125/360 (34.7%) in transversal plane, and in 105/504 (20.8%) – in auditory handicapped children. According to the age, the most affected was the age group of 12-15 y.o.: 467/1388 (33.7%) of children, the group of 9-12 y.o. – 393/1388 (28.3%) of children, and 7-9 y.o. group – 314/1388 (22.6%) of children.
Conclusions. Muscle spasticity in physically, visually and auditory disorders children can be considered as key predictors and risk factors in the appearance of malocclusion in children. Children with special needs may be treated according to the age and the nature of malocclusion
Keywords: malocclusion, children, special care needs, orthodontic treatment.
INTRODUCTION
The wide range of malocclusion is due to anatomical-topographic features of the maxilla in children with different age. It is known that children with special needs have a higher frequency and more severely develop both the clinic and imagistic features of malocclusions. As a part of dental medical practice malocclusion in children with special needs at different age has become a subject of study of several scientific fields such as maxilla-facial surgery, orthodontic, restorative dentistry, neurology and genetics.
At the same time the various need for orthodontic treatment increase in these children. According to the Birgit Th. (2001), this increase turns out to be based on the child’s age. Thus, at the age 12-15 years old children according to the type of malocclusions, it reaches a level of 24.4% of children [1, 2].
The assessment of morbidity of malocclusions remains one of the major concerns of pediatric dental medical services because the early detection of these problems is the basic component of effective prophylaxis. In adults, untreated cases in childhood are maintained in different complications forms [3, 4].
The recognition of the new cases depends on the diagnosis of the orthodontic care system and on the choice of orthodontic criteria [5, 6]. Epidemiological researches have increased particularly in recent years [7, 8].
Evaluation of the incidence and prevalence of malocclusions reveals the fact with age in children increases the probability of worsening the state of dental system by unbalanced occlusion [9, 10]. It can serve as an important method to distinguish different etiological factors. For example, the lack of variability of malocclusion is an indicator of many genetic features. While others involve nongenetic factors in existence of many variables malocclusions [11].
The continuous improvement of examination methods and their extension over large population, especially their accessibility at the child’s age, make it possible to evaluate a wide range of pathological entities often associated and masked [12].
The environmental factors play an important role in accentuating or limiting these existing malocclusions. An early orthodontic treatment can positively influence on the development of these malocclusions.
The orthodontic problems that remain to be resolved are to determine which of the various pathological entities are due to genetic differences and which depend on the environmental factors. Preventing and treating these malocclusions requires a knowledge of the etiological factors [13, 14, 15].
In this context, the aim of the study was to determine the incidence of the malocclusions in children with special needs at different ages in the process of social adaptation. Another objective of the research was to evaluate the degree of association between different types of malocclusions in a sagittal, vertical and transversal plane and children with auditory, visually and physical disorders in order to optimize orthodontic treatment.
MATERIAL ȘI METHODS
Epidemiological research was made in the period of 2016-2017 years and included children with special needs from orphanages, auxiliary schools and special gymnasiums for visually, auditory and physically handicapped children
The study protocol was approved by the Research Ethics Committee of the Nicolae Testemitanu SUMPh (minutes no. 42 from 14.12.2016). Data collection was possible, based on the permission of the Ministry of Health of Republic of Moldova and of the Direction for protection of the child’s rights.
As inclusion criteria were: children during mixed dentition and early permanent dentition not following orthodontic treatment. The research didn’t include children growing up in a familiar environment, children with temporary dentition, children with cleft palate and lip, children who were in orthodontic treatment.
The orthodontic examination was performed in a private room. The children were seated in the chair with the head fixed in the vertical position and included the following types of tools disposable dental mirror, chemical pencil, wooden spatula, caliper, portable light.
For the assessment of malocclusions, it was used Bjӧrk and coll. method (1964, 1972) [6]. Malocclusions were assessed in sagittal, vertical and transversal planes.
The measurement overjet and reverse overjet was made with the aid of millimeter graded ruler and measured the distance from the most prominent surface of the labial surface of the upper central incisor and the labial surface of the lower central incisor in centric occlusion (Figure 1a).
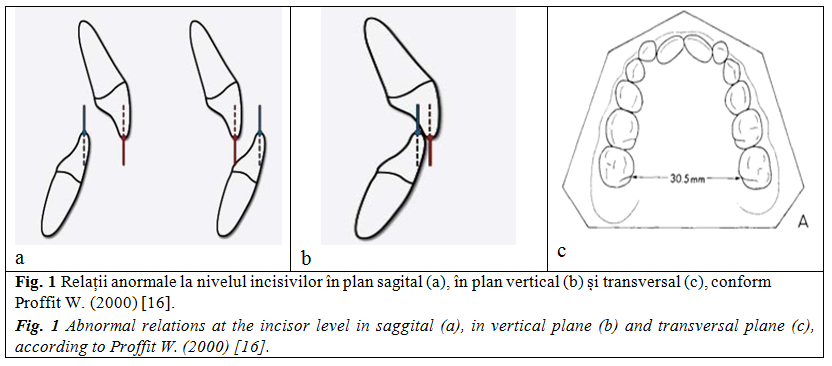
The overbite and open bite were measured while the subject in centric occlusion. The amount of vertical overlap of the upper incisor on the lower incisor is marked with a pencil on the labial surface of the lower incisor using the incisor edge of the upper incisor to guide the pencil with the sharpened point of the pencil itself parallel to the subject’s occlusal plane. In the case of an open bite, the amount of open bite is measured directly and recorded to the nearest whole millimeter (Figure 1b).
Anterior open bite was recorded in which one, two or three of the upper incisor occlude lingual to the lowers. Posterior crossbite was also recorded according to Bjork A., Skieller V. (1972), for each side for canine and premolar section and for molar section when the buccal cusp of the upper tooth occludes lingual to the buccal cusp of the corresponding lower tooth as well as midline deviation (Figure 1c). The measured parameters were recorded in the context of the persistence of abnormal relations at the incisor level in the sagittal plane (a), vertical plane (b) and transversal plane in auditory, visually and physically handicapped children.
The statistical analysis was done using the software STATISTICA 8.0. The qualitative variables were compared using Chi-square test. Data are presented as absolute (relative) values or as mean and standard deviation. The significant value for p was considered <0.05.
RESULTS
The prevalence of malocclusions among the examinated children was 67.5% (1388/2057 of examined children). From 1388 children, 812 (58.5%) were boys and 576 (41.5%) – girls (χ2=79.6; p<0.0001). According to Bjork and coll., have been highlighted three groups of the children with malocclusions:
a. in sagittal plane – 283/1388 (20.4%) children. Of these, 105/283 (37.1%) had auditory disorders, 91/283 (32.2%) had visual disorders, and 87/283 (30.7% ) – physical disorders;
b. in vertical plane – 741 (53.4%) children. Of these, 309/741 (41.7%) had physical disorders, 288/741 (38.9%) – auditory disorders, and 144/741 (19.4%) – visual disorders;
c. in transversal plane – 364/1388 (26.2%) children. Of these, 128/364 (35.2%) had physical disorders, 111/364 (30.5%) – auditory disorders, and 125/364 (44.3%) – visual disorders.
Depending on standardized five age groups, malocclusions in children with special needs were distributed as following: younger than 7 y.o. – 56/1388 (4.0%); 7-9 y.o. – 393/1388 (28.3%); 9-12 y.o. – 393/1388 (28.3%); 12-15 y.o – 467/1388 (33.7%) and older than 15 y.o. – 158/1388 (11.4%) of children.
The average age of male patients at the time of diagnosis of malocclusions was 9.8±0.3 years, and females` age was 13.8±0.7 years at the time of diagnosis (p=0.08).
A slightly increased malocclusion rate was found in urban dwellers (59.4%), compared to the rural dwellers (48.5%).
The distribution of dentomaxillary abnormalities in children with special needs is presented in Table 1. It is easy to see that the prevalence of comorbidity factors (vision, hearing or motor disorders) is high and variable in different patient groups.
 In the group of children with special needs assessed a high frequency of malocclusions in the sagittal plane, especially maxillary overjet. The proportions of maxillary overjet, deep bite and crossbite varied significantly depending on the type of children’s disability, while reverse overjet, open bite and midline deviation had a relatively stable proportion (Table 2).
In the group of children with special needs assessed a high frequency of malocclusions in the sagittal plane, especially maxillary overjet. The proportions of maxillary overjet, deep bite and crossbite varied significantly depending on the type of children’s disability, while reverse overjet, open bite and midline deviation had a relatively stable proportion (Table 2).
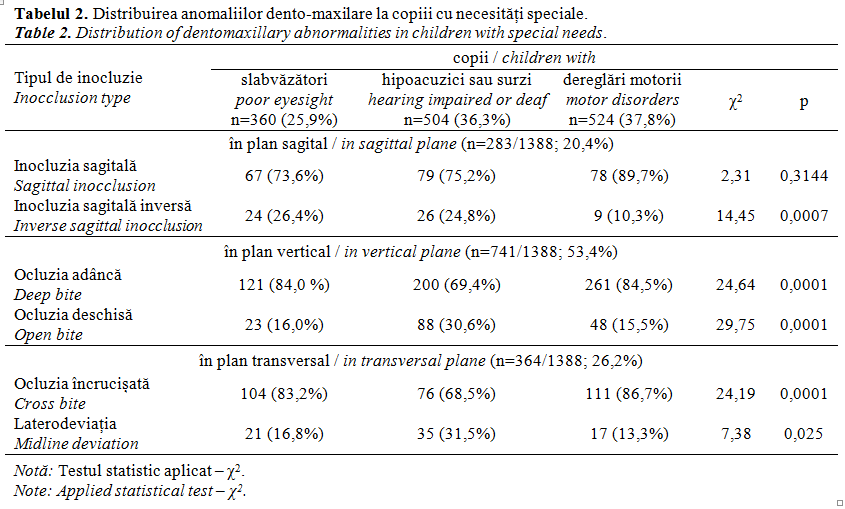
In vertical dentomaxillary anomalies in children with special needs, deep occlusion prevails over open occlusion. The deep occlusion was characteristic for patients with motor disorders (84.5%) and poor vision – 84.0% of the cases (Table 2).
Crossbite showed a significant difference in children with special needs. Early loss of temporary teeth due to neglect and lack of dental treatment as well as accidental loss of the teeth led to their movement to the left, right, space closing for permanent teeth thus, deviate the mandible to the left or right mainly in children with physical (13.3%) and visually (16.8%), disorders and more in children with auditory (31.5%) disorders (Table 2).
Children with special needs are considered normal children who may be receiving early treatment for space-maintaining or could benefit from a removable appliance to regain space. An effective control of malocclusions among children with visually, auditory and physical disorders will still require good interdisciplinary approach.
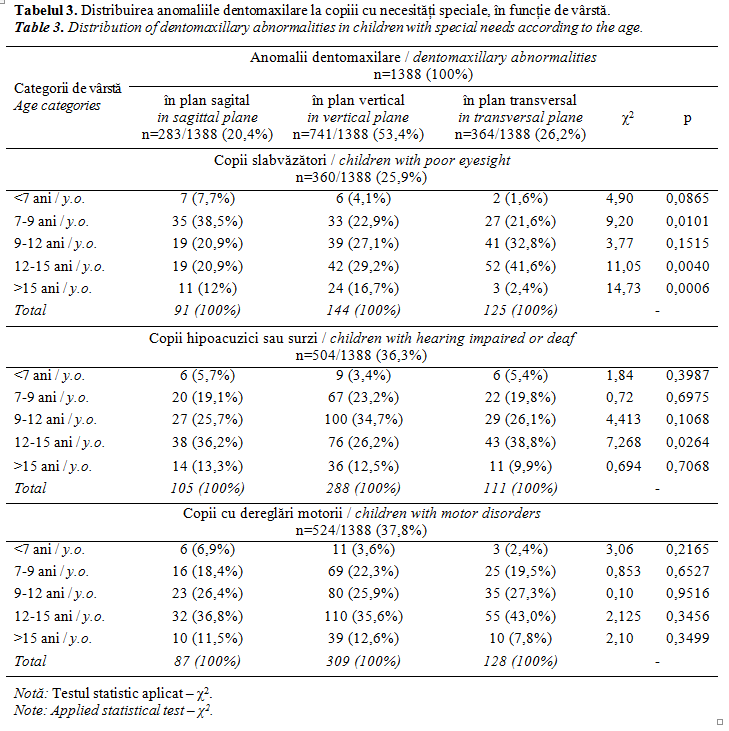
From the study, the prevalence of dentomaxillary anomalies in the vertical and transverse planes is evident in children with vision disorders at the age of 12-15 years, compared with those aged 9-12 years and 7-9 years. While the dentomaxillary anomalies in the sagittal plane, on the contrary, prevailed at the age of 7-9 years compared to other age groups. Vertical dentomaxillary abnormalities in children with hearing loss or deafness were more frequent at the age of 9-12 years, compared to other groups. However, in children with motor disorders, in all age periods, dentomaxillary abnormalities predominated vertically. Sagittal abnormalities predominated at the age of 7-9 years, whereas transverse abnormalities were more frequent in children 12-15 years (Table 3).
DISCUSSION
In vertical dentomaxillary anomalies in children with special needs, deep occlusion prevails over open occlusion. The deep occlusion was characteristic for patients with motor disorders (84.5%) and poor vision – 84.0% of the cases (Table 2).
Crossbite showed a significant difference in children with special needs. Early loss of temporary teeth due to neglect and lack of dental treatment as well as accidental loss of the teeth led to their movement to the left, right, space closing for permanent teeth thus, deviate the mandible to the left or right mainly in children with physical (13.3%) and visually (16.8%), disorders and more in children with auditory (31.5%) disorders (Table 2).
Children with special needs are considered normal children who may be receiving early treatment for space-maintaining or could benefit from a removable appliance to regain space. An effective control of malocclusions among children with visually, auditory and physical disorders will still require good interdisciplinary approach.
From the study, the prevalence of dentomaxillary anomalies in the vertical and transverse planes is evident in children with vision disorders at the age of 12-15 years, compared with those aged 9-12 years and 7-9 years. While the dentomaxillary anomalies in the sagittal plane, on the contrary, prevailed at the age of 7-9 years compared to other age groups. Vertical dentomaxillary abnormalities in children with hearing loss or deafness were more frequent at the age of 9-12 years, compared to other groups. However, in children with motor disorders, in all age periods, dentomaxillary abnormalities predominated vertically. Sagittal abnormalities predominated at the age of 7-9 years, whereas transverse abnormalities were more frequent in children 12-15 years (Table 3).
CONCLUSION
- More often malocclusions have been seen in children with physical disorders due to non-coordination of movements both at the body and at the mandibular level by disordering masticatory function compare to the children with visually and auditory disorders.
- Malocclusions in transversal plane, namely cross bite, have been seen in children with physical disorders. But this can be associated with midline deviation, especially in children with visually disorders.
- The frequency of dentomaxillary anomalies in children with special needs was significantly more common in boys than in girls.
Declaration of conflicting interests
The authors mention no conflicts of interest.
Author’s contribution
The authors have participated equally in design of the study, data collection, in writing of the article. The authors have read and finally version being accepted.
REFERENCES
- Birgit T., Lucia P., Clementina I. et al. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. European Journal of Orthodontics, 2001; 23 (2): 153-166.
- Bjork A., Skiller V. Facial development and tooth eruption. Am. J. Orthod., 1972; 62 (4): 339.
- Celikoglu M., Akpinar S., Yavuz I. The pattern of malocclusion in a sample of orthodontic patients from Turkey. Med. Oral Patol. Oral Cir. Bucal., 2010; 15 (5): 791-796.
- Zegan G. Ortodonție și ortopedie dentofacială. Iași: Editura Tehnopress, 2005.
- Aynar T., Galan A.F., Marin I., Dominguez A. Dental arch diameters and relationships to oral habits. Angle Orthod., 2006; 76 (3): 441-445.
- Björk A., Krebs A., Solow B. A method for epidemiological registration of malocclusion. Acta Odontologica Scandinavica, 1964; 22: 27-41.
- Souza D., Semeghini T., Kroll L., Berzin F. Oral myofunctional and electromyografic evaluation of the orbicularis oris and mentalis muscles in patients with class II/1 malocclusion submitted to first premolar extraction. J. Appl. Oral Sci., 2008; 16 (3): 226-231.
- Bhayya D., Shyagali T., Dixit U. Study of occlusal characteristics of primary dentition and the prevalence of malocclusion in 4 to 6 years old children in India. Dent. Res. J. (Isfahan), 2012; 9 (5): 619-623.
- Carvalho A., Paiva S., Viegas C. et al. Impact of malocclusion on oral health-related quality of life among brazilian preschool children: a population-based study. Braz. Dent. J., 2013; 24 (6): 655-661.
- Dorobăț V., Stanciu D. Ortodonție și ortopedie dentofacială. București: Editura Medicală, 2011.
- Vernon M. Fifty years of research on the intelligence of deaf and hard of hearing children: review of literature and discussion of implications. Journal of Deaf Studies and Deaf Education, 2005; 10 (3): 252-260.
- Lin J., Gu Y. Preliminary investigation of nonsurgical treatment of severe skeletal Class III malocclusion in the permanent dentition. Angle Orthod., 2003; 73: 401-410.
- Cattoni D., Fernandes F. Facial measurements and proportions in children: contributions to orofacial myofunctional evaluation. Pro fono, 2004; 16 (1): 7-18.
- Drevensek M., Papic J. The influence of the respiration disturbances on the growth and the development of the orofacial complex. Coll. Antropol., 2005; 29 (1): 221-225.
- Menzes V., Leal R., Moura M. et al. Influence of socio-economic and demographic factors in determining breathing patterns: a pilot study. Rev. Bras. Otorhinolaringol., 2007; 73 (6): 826-834.
- Proffit W. Contemporary Orthodontics. 2th edition. St. Louis: Mosby Co, 2000.
- Lessa F., Enoki C., Ferres M. et al. Breathing mode influence in craniofacial development. Rev. Bras. Otorhinolaringol, 2005; 71 (2): 156-160.
- Hayder S. Al-Atabi, Fakhri Abid Ali. Prevalence of malocclusion in mentally, physically, auditory and visually handicapped patients in Sammawa City aged years old. J. Bagh College Dentistry, 2011; 23 (1): 107-111.
- Lopatiene K., Babarskas A. Malocclusion and upper obstruction. Medicina, 2002; 38 (3): 277-283.
- Menzes V., Leal B., Pessoa R., Pontes R. Prevalence and factors related to mouth breathing in school children at the Santo Amaro project – Recife 2005. Rev. Bras. Otorhinolaringol., 2006; 72 (3): 394-399.
- Sousa R., Pinto-Monteiro A., Martins C. et al. Malocclusion and socioeconomic indicators in primary dentition. Braz. Oral Res., 2013; 28 (1): 54-60.
- Valera F., Travitzki L., Matta S. et al. Muscular, functional and orthodontic changes in preschool with enlarged adenoids and tonsils. Int. J. Pediatr. Otorhinolaryngol., 2003; 67 (7): 761-770.
- Yata R., Motegi E., Ueda K. et al. A lip seal study of Japanese children with malocclusion. Bull. Tokyo Dent. Coll., 2001; 42 (2): 73-78.